

Preparing aged-care facilities for assessor-led funding under AN-ACC
Telstra Health’s Clinical Manager is a core operational system used daily by residential aged-care providers to manage clinical documentation, administration, and compliance. It sits at the centre of how care is recorded, evidence is assembled, and regulatory obligations are met.
Following the Royal Commission into Aged Care Quality and Safety, funding reform replaced ACFI with AN-ACC and changed how resident classifications are determined. Providers no longer determine funding outcomes but remain responsible for the quality and completeness of evidence reviewed by independent assessors. This work updated Clinical Manager to support assessor-aligned preparation workflows within that shift.
Clinical Manager operates across a national footprint of approximately 60,000 residential aged-care beds, situating this system update within a large-scale AN-ACC funding and compliance environment.
At a glance
System shift: System shift: From provider-led funding calculation to assessor-aligned preparation
Capability: Evidence traceability organised by national assessment structure
Scope: Assessment preparation embedded within a live, legacy care platform
Operating environment
Context
Organisation: Telstra Health (Aged & Disability)
Environment: Residential aged-care software platform (Clinical Manager)
Users: Clerical and clinical staff preparing residents for assessment
Role: Senior UX Designer
Timeframe: 6-month delivery window
Constraints
Government-defined funding and assessment model
Classification authority external to providers
Long-established platform with embedded legacy workflows
High audit and compliance exposure
Assessment authority shifted outside facilities
PART 1
Policy context
The Royal Commission identified systemic issues in aged-care funding, including inconsistent classification practices and incentives misaligned with resident need. In response, the Australian Government replaced ACFI with AN-ACC to standardise assessment nationally and remove funding determination from providers.
This was not a product change.
It was a structural shift in responsibility and accountability.
The ACFI operating model
Under ACFI:
Assessments were completed internally.
Evidence was collected, scored, and reviewed in-house.
Funding outcomes could be estimated using a calculator.
Scoring logic was visible to providers.
This transparency shaped behaviour. Because outcomes could be anticipated, preparation practices aligned to known scoring mechanics. During the Royal Commission, this dynamic was cited as a risk to equity and consistency, including optimisation around residents aligned to higher funding bands.
Clinical Manager reflected this model through calculator-led workflows and score-driven interpretation.
What AN-ACC changed
AN-ACC shifted assessment responsibility away from providers.
Under the new model:
Independent assessors apply a national assessment tool.
Classifications are no longer determined internally.
Funding depends on assessor interpretation of submitted evidence.
Classification logic is not visible to providers.
Internal systems shifted from assessment to preparation.
Early interviews with service managers highlighted concern about funding risk, assessor interpretation, and whether existing documentation would be sufficient under external review.
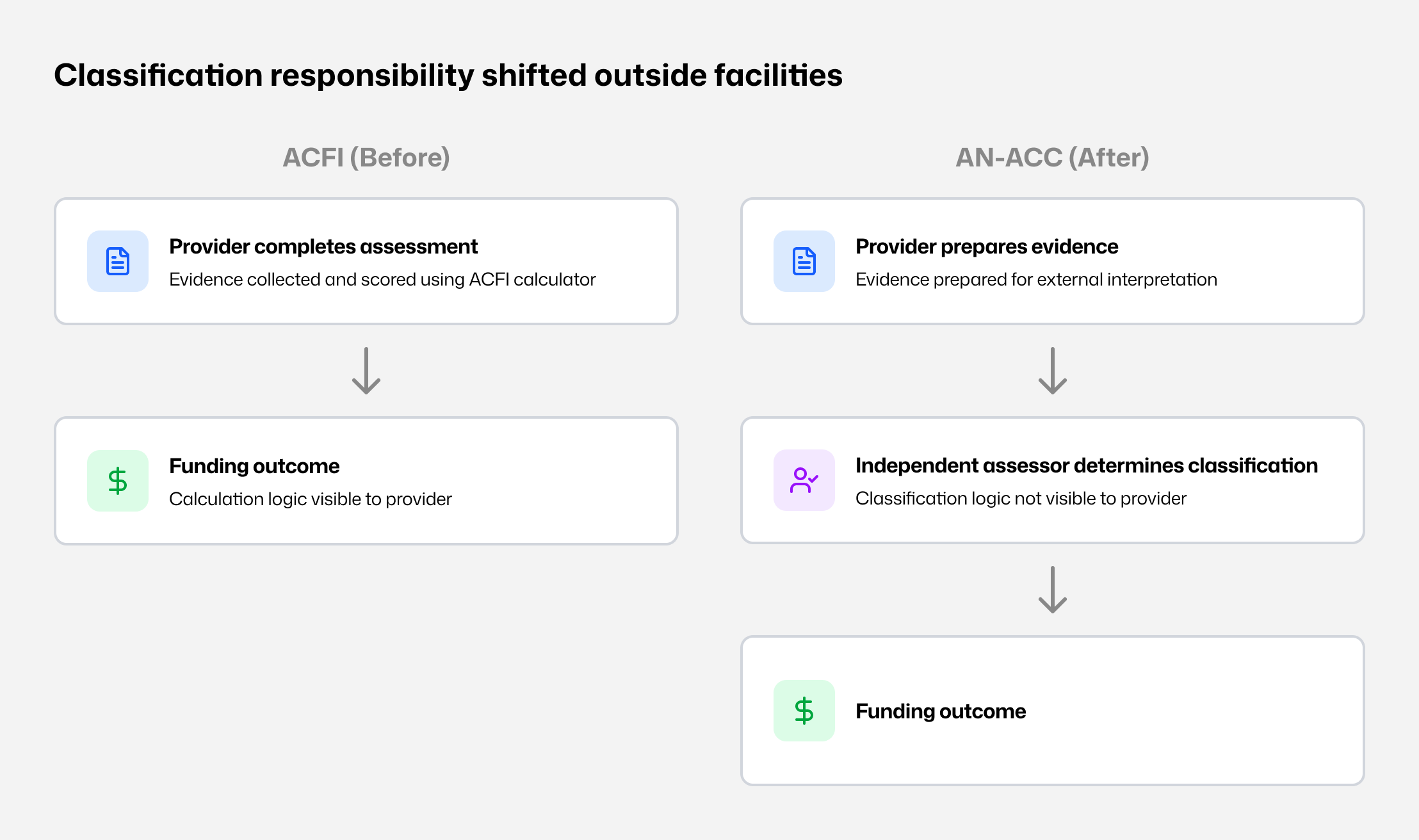
Classification shift - Assessment moved from provider-led scoring to external classification.
Loss of calculation visibility
At rollout, the logic used by assessors to determine classifications was not available to providers. Preparation quality now depended on whether assessors could:
locate relevant evidence,
understand its context, and
interpret resident need accurately.
This increased the importance of structured, complete, and easily retrievable evidence.
Resulting system mismatch
Within Clinical Manager:
Existing workflows reinforced a scoring mindset that no longer applied.
Evidence existed across notes, charts, and forms but was not organised by assessment section.
Calculator patterns implied predictability and control that providers no longer had.
The primary risk was not usability.
It was preparing staff for a process that no longer existed.
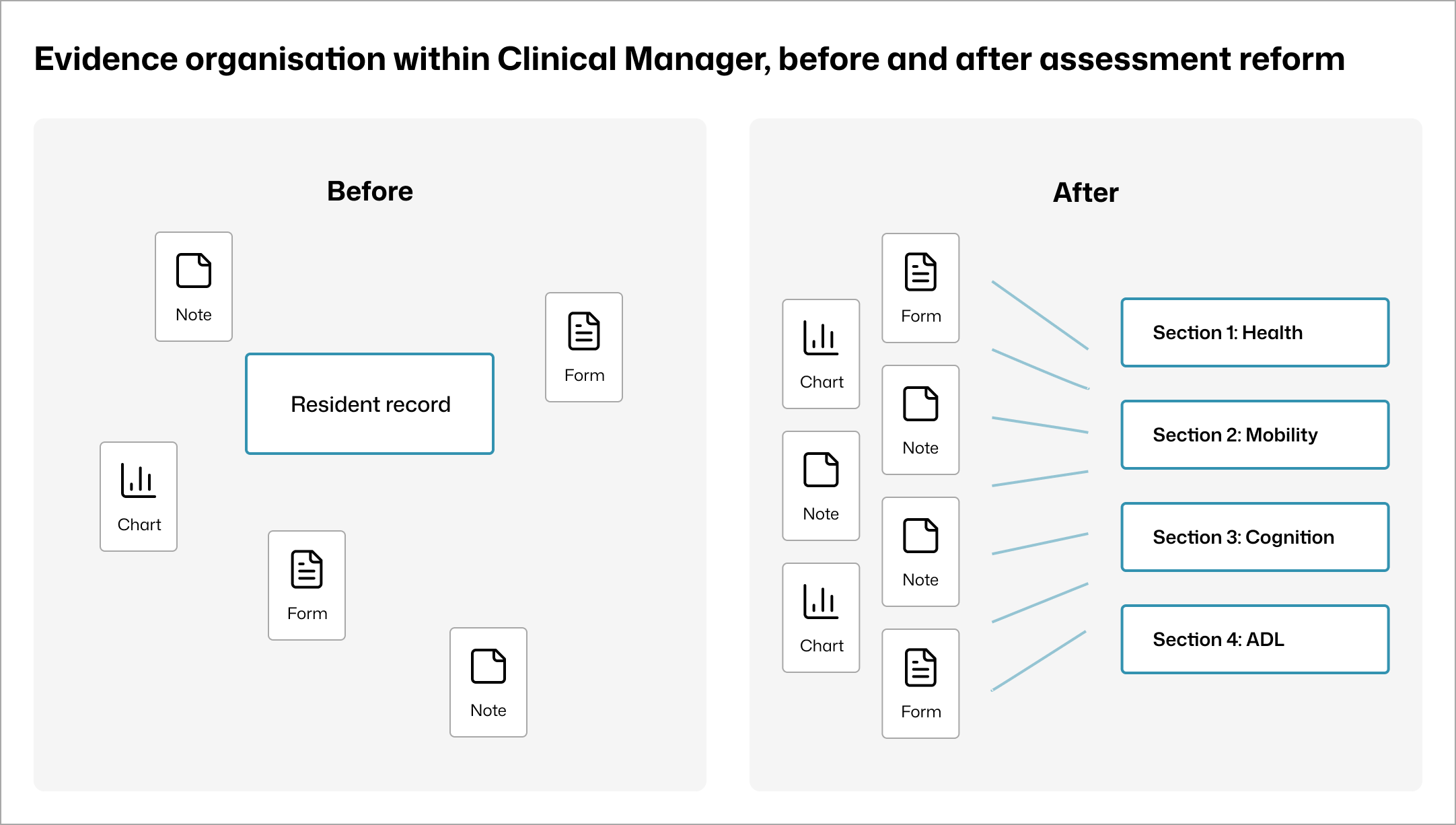
Evidence storage before and after -Documentation existed but was not organised by AN-ACC sections.
Insight
Staff were not seeking to influence outcomes. They wanted clarity on how to prepare evidence that would withstand external review.
Shaping a preparation system aligned to assessor interpretation
PART 2
System intent
Before interface decisions, the system boundary was made explicit.
The system would:
support preparation for assessment,
reflect the AN-ACC assessment structure,
surface evidence in assessment context.
The system would not:
determine classifications,
predict funding outcomes,
reproduce ACFI optimisation patterns.
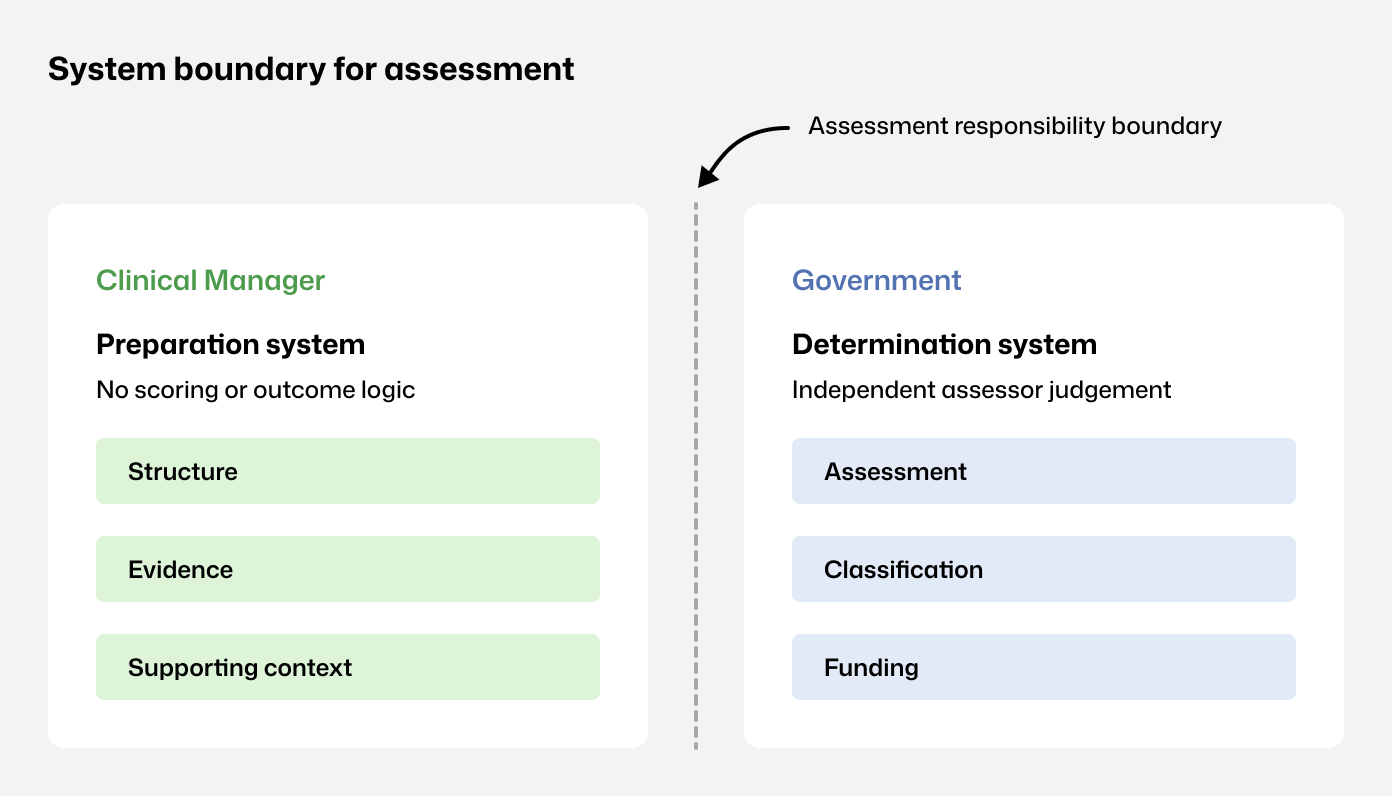
Assessment boundaries - Clinical Manager supports preparation; assessment and funding sit externally.
Structural decisions
Decision: Avoid optimisation patterns that imply control over classification.
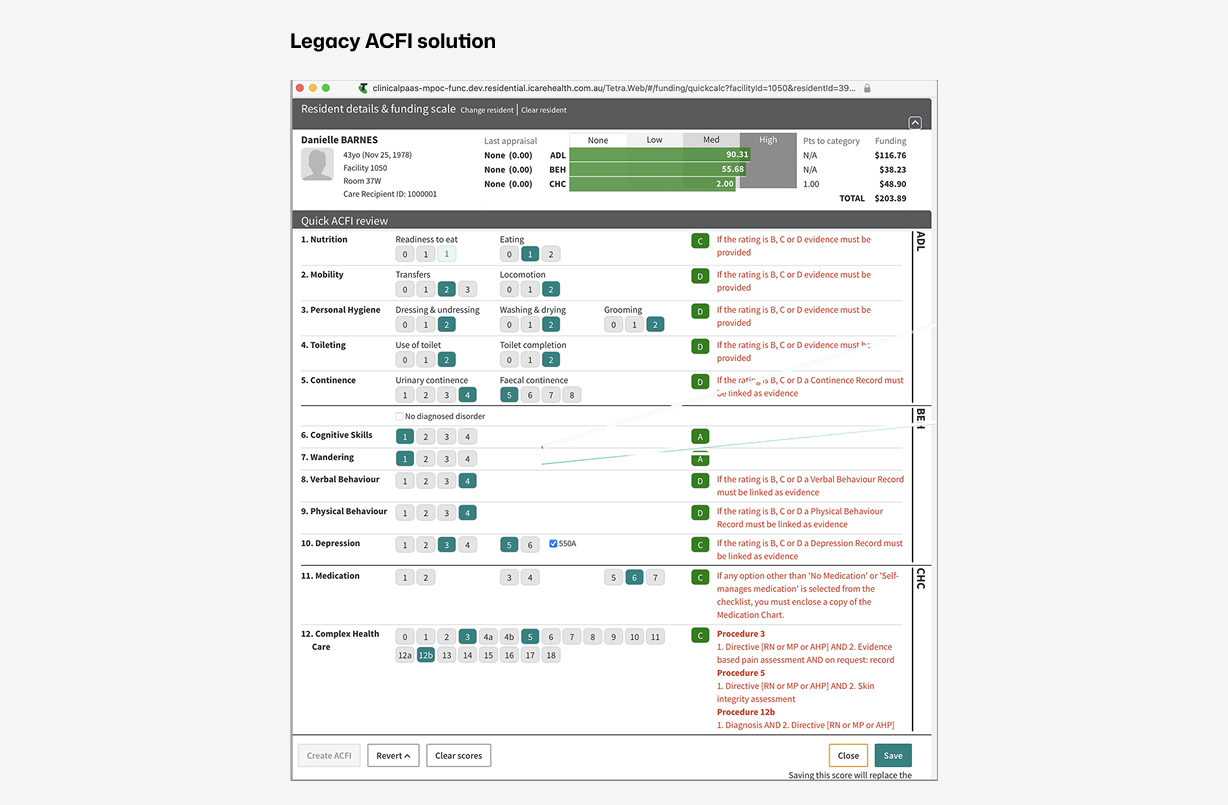
ACFI calculator -Calculator-led workflows reinforced internal scoring.
Decision
Do not reproduce funding calculators or prediction logic inside Clinical Manager.
Decision: Use AN-ACC instruments as the primary information architecture.
Assessment navigation mirrored the national instrument structure, creating a shared definition of completeness and reducing missed sections.
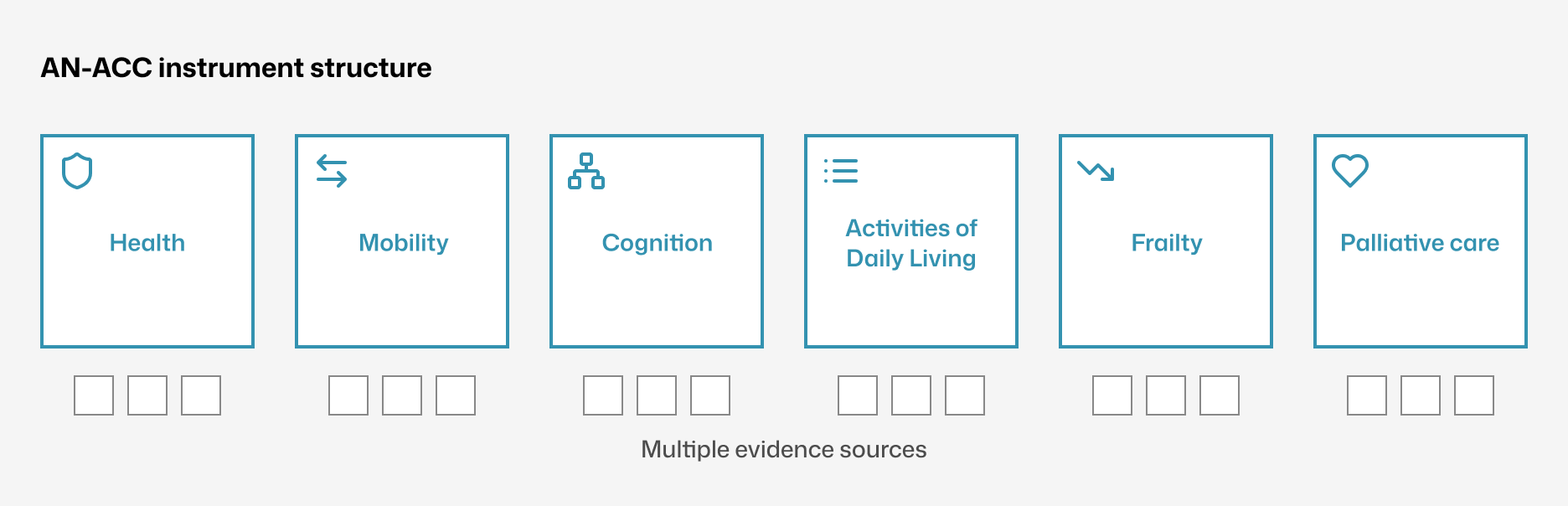
Structure to follow AN-ACC instrument - Navigation mirrors the AN-ACC structure.
Decision: Link evidence at the assessment-section level.
Evidence remained part of the resident record while becoming explicitly linkable to assessment sections, enabling traceability without duplication.
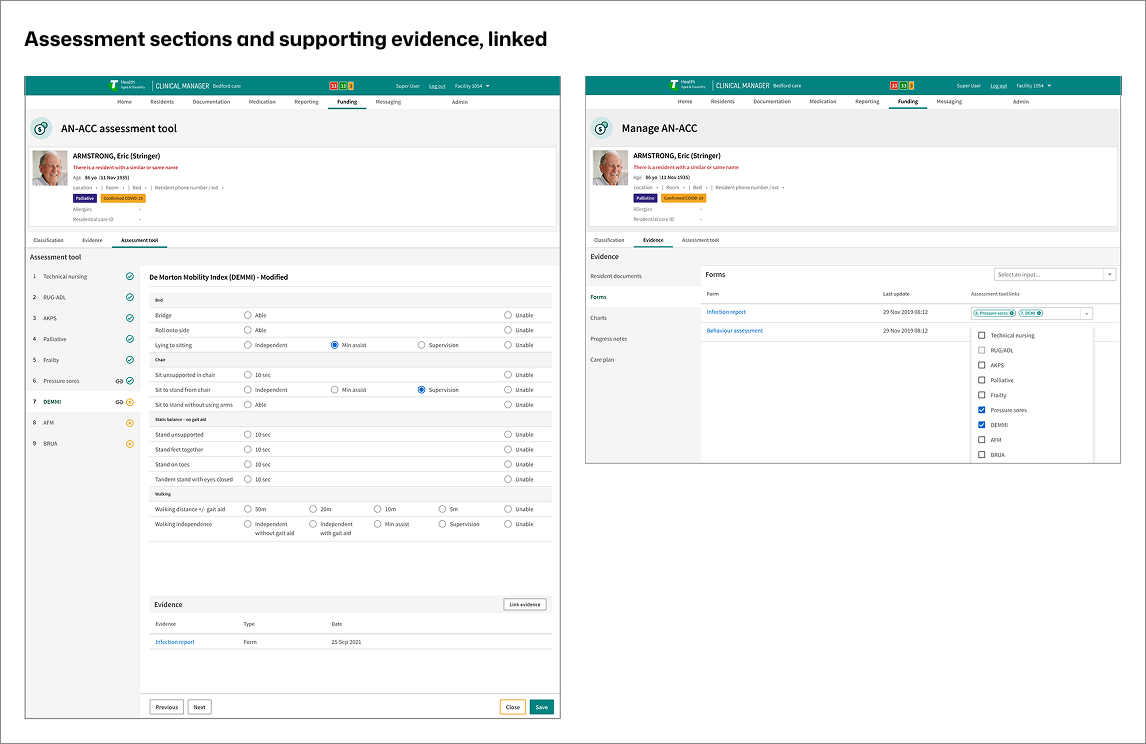
Direct link to supporting evidence -Evidence is linked to assessment sections without duplication.
User experience prioritisation
Predictability governed the UX:
stable navigation by assessment section,
consistent layouts across instruments,
visible evidence status in context,
linear progression over branching.
This reduced decision load while staff continued routine care.
What was rejected
Facility-side scoring or funding prediction tools
Free-form evidence repositories detached from assessment structure
Parallel funding packs outside the resident record
Global evidence visibility without role-based controls
Each weakened traceability or implied outcome control, conflicting with AN-ACC’s separation of preparation and determination.
Capability created and supporting evidence
PART 3
Capability created
Assessor-aligned preparation structure inside Clinical Manager
Clear separation between preparation and external determination
Evidence
Structural impact:
One preparation flow replaced four to five disconnected screens
Assessment sections and linked evidence presented together
Increased staff confidence during readiness activities
Measured outcomes:
Evidence lookup time reduced by~70% (6–10 min to under 2 min)
Reduced follow-up clarification after preparation
What was not proven
Classification accuracy
Funding outcomes
Long-term documentation behaviour change
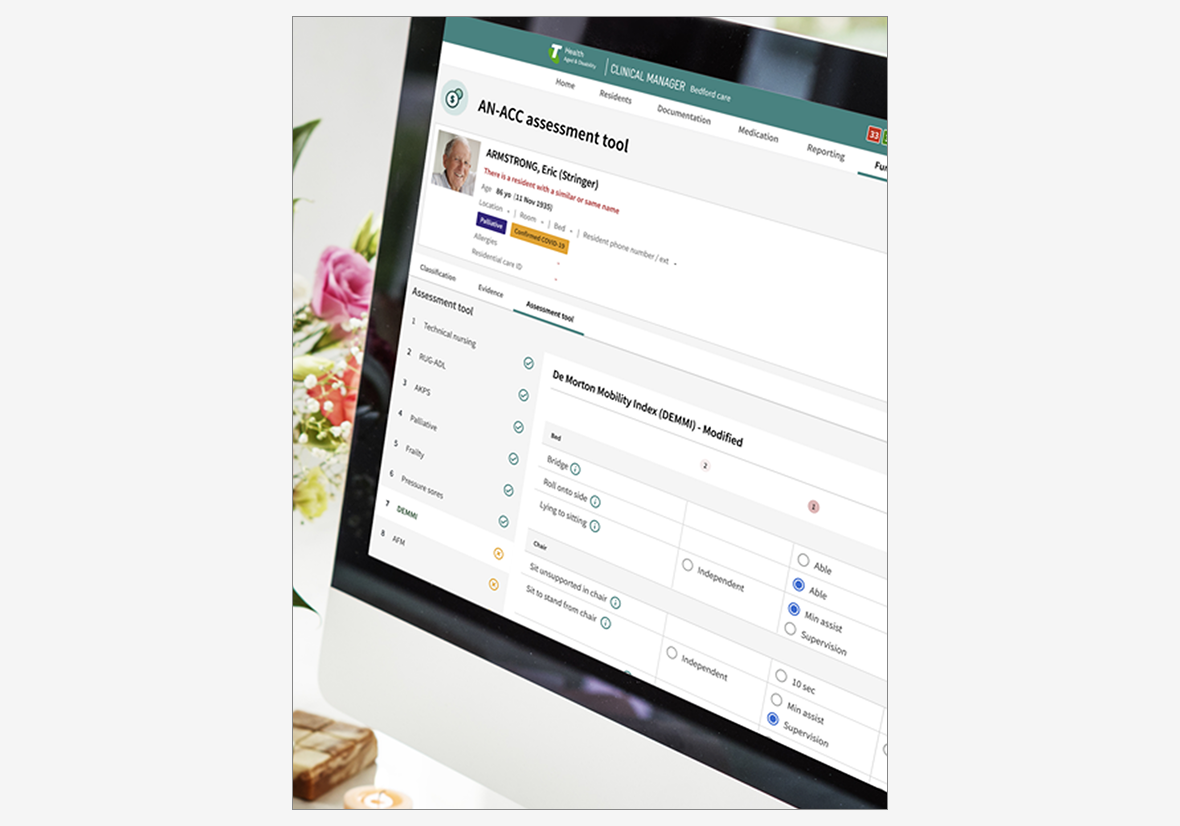
AN-ACC funding portal within Clinical Manager - Interface showing how evidence is organised by assessment section within the live Clinical Manager environment.
Outcome
Facilities regained control over preparation quality without implying control over classification outcomes.
Reflection
AN-ACC reframed funding preparation as an evidence and interpretation problem.
By aligning system structure to the assessor lens and making evidence explicit within the resident record, Clinical Manager implemented a preparation model capable of supporting reform-driven change without reworking underlying care workflows.